Chronic Inflammatory Demyelinating Polyradiculoneuropathy
What is chronic inflammatory demyelinating polyradiculoneuropathy?
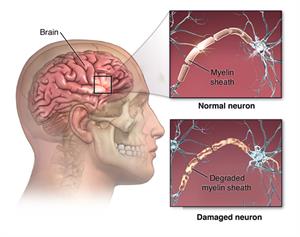
Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) is a rare type of autoimmune disorder. In an autoimmune disease, the body attacks its own tissues. In CIDP, the body attacks the myelin sheaths. These are the fatty coverings on the fibers that insulate and protect the nerves.
Experts think that CIDP is related to the more commonly known disease Guillain-Barré syndrome (GBS). GBS is generally considered a short-term (acute) disease. CIDP is considered a long-term (chronic) disease. CIDP is less common than GBS.
CIDP is usually classified as follows:
-
Progressive. The disease continues to get worse over time.
-
Recurrent. Episodes of symptoms stop and start.
-
Monophasic. This means one bout of the disease lasts 1 to 3 years and doesn’t happen again.
What causes CIDP?
CIDP occurs when the body's immune system attacks the myelin sheaths around nerve cells in the peripheral nervous system. These are the nerves outside the brain and spinal cord. But exactly what sets this off isn't clear. Unlike GBS, there usually isn't an infection preceding CIDP. There doesn't seem to be a genetic link to CIDP.
Who is at risk for CIDP?
CIDP can occur in anyone. But people in their 50s and 60s seem more likely to develop it than people in other age groups. Men are twice as likely as women to get the disease.
What are the symptoms of CIDP?
Symptoms are usually the same for all types of CIDP. They can include:
-
Tingling in the arms and legs
-
Gradual weakening of the arms and legs
-
Loss of reflexes
-
Loss of balance and your ability to walk
-
Loss of feeling in the arms and legs, which often starts with not being able to feel a pinprick
How is CIDP diagnosed?
Because CIDP is rare, it’s often hard to correctly diagnose the disease, at least at first. Healthcare providers can confuse its symptoms with those of GBS because of the similarity between the diseases. If symptoms last longer than 8 weeks, a provider may suspect CIDP.
After taking a medical history and doing a physical and neurological exam, a healthcare provider may do two or more tests to confirm a diagnosis. These may include:
-
Blood and urine tests
-
A nerve conduction study and electromyography to look for myelin damage in peripheral nerves. This involves using mild electrical currents to test nerve and muscle function and response.
-
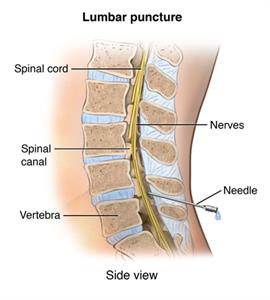
A lumbar puncture to see if levels of certain proteins related to the disease are higher than normal. To do this, a small needle is inserted into the back and a small amount of the fluid that surrounds the spinal cord (cerebrospinal fluid) is withdrawn.
-
A nerve biopsy to look at microscopic changes in the nerves. This test is rarely done.
-
MRI may show inflammation of the nerve roots. The roots are the part of the nerve where it branches off from the spinal cord.
 |
| PNerv_20140304_v0_002 |
How is CIDP treated?
Treatment for CIDP is often effective. Some studies show that up to 4 in 5 people respond well to therapy. Because it's an autoimmune disorder, healthcare providers use medicines that suppress the immune response to treat CIDP. Medical teams tailor your treatment to each person and closely keep track of their progress. Treatments for CIDP include:
-
Immunosuppressive medicines
-
Steroids
-
Intravenous or subcutaneous immunoglobulin
-
Plasma exchange (plasmapheresis)
-
Monoclonal antibody therapy
Living with CIDP
The course of CIDP can vary greatly among people, as can the response to treatment.
Getting treatment as early as possible is very important because it gives them the best chance of limiting symptoms and keeping this condition under control. If they don't seek treatment for CIDP, symptoms will likely get worse over the course of months to several years. These can range from sensory symptoms, such as tingling and numbness, to weakness and loss of balance. Without treatment, 1 in 3 people with CIDP will need a wheelchair.
In people with any physical impairments, physical therapy can be very important. In this treatment, specialists work with them to maintain or increase strength and improve coordination. Another type of therapy is occupational therapy. It helps people learn new ways of doing everyday tasks in spite of new physical limitations.
Some people with physical disabilities often feel sad or depressed. If this happens, a healthcare provider may recommend seeing a mental health provider. Antidepressants and psychotherapy can help treat depression. So can support groups for people managing chronic health conditions.
When should I call my healthcare provider?
If you have been diagnosed with CIDP, talk with your healthcare provider about when you might need to call them. They'll likely advise you to call if you notice any symptoms getting worse or if you develop any new symptoms.
Key points about CIDP
-
Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) is a slowly developing autoimmune disorder in which the body's immune system attacks the myelin that insulates and protects the body’s nerves. The exact cause isn't known.
-
Common symptoms are gradual weakness or sensation changes in the arms or legs. This might get worse over time, or it might come and go.
-
Early treatment is important to limit disease progression. It includes medicines or other treatments to suppress the immune system.
Next steps
Tips to help you get the most from a visit to your healthcare provider:
-
Know the reason for your visit and what you want to happen.
-
Before your visit, write down questions you want answered.
-
Bring someone with you to help you ask questions and remember what your provider tells you.
-
At the visit, write down the name of a new diagnosis and any new medicines, treatments, or tests. Also write down any new instructions your provider gives you.
-
Know why a new medicine or treatment is prescribed, and how it will help you. Also know what the side effects are.
-
Ask if your condition can be treated in other ways.
-
Know why a test or procedure is recommended and what the results could mean.
-
Know what to expect if you do not take the medicine or have the test or procedure.
-
If you have a follow-up appointment, write down the date, time, and purpose for that visit.
-
Know how you can contact your healthcare provider if you have questions, especially after office hours or on weekends and holidays.