When Your Child Has Aortic Stenosis (AS)
The heart is divided into 4 chambers. The 2 upper chambers are called atria. The 2 lower chambers are called ventricles. The heart contains 4 valves. The valves open and close to keep blood flowing forward through the heart. The aortic valve is between the left ventricle and the aorta. It has 3 leaflets that open and close to allow blood through. It controls the flow of blood from the heart to the rest of the body (except for the lungs). Aortic stenosis (AS) is when this valve doesn’t open all the way. This may occur when the valve leaflets are fused together. Or it may happen if there are only 1 or 2 leaflets present instead of the normal 3. It can also occur when the area above or below the valve is too narrow. As a result, blood flow from the heart to the rest of the body is blocked. If not treated, this condition can lead to heart problems over time. But treatment can often be done.
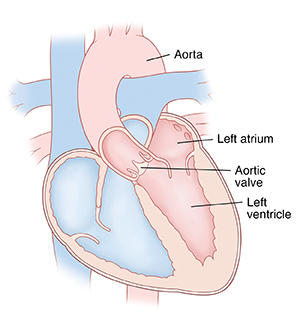 |
| Inside view of a normal heart showing the left heart structures |
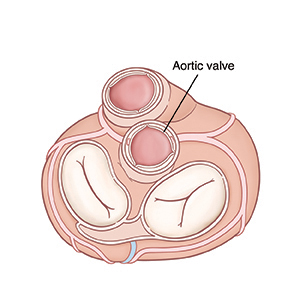 |
| Top view of heart. |
Types of aortic stenosis
AS comes in different types. They are:
-
Supravalvar. This is when blockage occurs above the valve. The aorta may be too narrow.
-
Valvar. This is when blockage occurs at the valve. The leaflets may be too thick, stuck together, or 1 or more leaflets may be missing.
-
Subvalvar. This is when blockage occurs below the valve. The area below the valve may be too narrow.
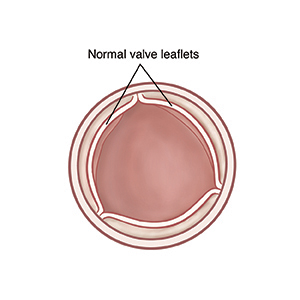 |
| An open normal aortic valve (view from above). |
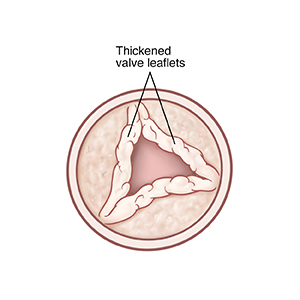 |
| An open aortic valve with stenosis. |
What causes aortic stenosis?
In most cases, AS is a congenital heart defect. This means that your child is born with this abnormal heart structure. It may be the only defect. Or it may be part of a more complex set of defects. The exact cause is unknown. But most cases seem to occur by chance. Having a family history of left-sided heart defects can be a risk factor.
Why is aortic stenosis a problem?
AS forces the left ventricle to work harder to pump blood through the aortic valve into the aorta to reach the body. This causes the left ventricle to thicken (hypertrophy) and get larger. Over time, the left ventricle can become so overworked that it no longer pumps blood well. This condition is known as heart failure (HF).
In severe cases of AS, blood flow to the coronary arteries can be reduced. This can cause chest pain or a heart attack.
Children with valve problems, such as AS, may be at risk of an infection of the inner lining of the heart or the heart valves. This is called infective endocarditis. Some people with aortic stenosis have other congenital problems, such as coarctation of the aorta.
What are the symptoms of aortic stenosis?
Children with mild or moderate AS may have no symptoms. Children with severe or critical AS will usually have symptoms. These can include:
In babies:
-
Trouble feeding
-
Poor growth
In older children:
How is aortic stenosis diagnosed?
During a physical exam, your child's healthcare provider checks for signs of a heart problem, such as a heart murmur. This is an extra noise caused when blood doesn’t flow smoothly through the heart. If your child's healthcare provider suspects a heart problem, they will refer you to a pediatric cardiologist. This is a healthcare provider who diagnoses and treats heart problems in children. Your child may have tests such as:
-
Chest X-ray. X-rays are used to take a picture of the heart and lungs.
-
Electrocardiogram (ECG). This test records the electrical activity of the heart.
-
Echocardiogram (echo). This test uses sound waves (ultrasound) to create pictures of the heart and look for structural defects.
-
Cardiac catheterization. In this test, your healthcare provider inserts a small, thin catheter into a large blood vessel and guides it to the heart where it is used to measure pressure in the aorta and heart.
How is aortic stenosis treated?
-
Mild or moderate AS often doesn't need treatment. But your child will need regular visits with a cardiologist. This is to make sure that narrowing at or near the valve doesn’t get worse over time.
-
Severe or critical AS needs treatment. Your child's healthcare provider may give medicines to keep the ductus arteriosus open until a procedure can be done. They may also prescribe other medicines to help relieve symptoms. More treatment will be needed to relieve the blockage and let blood flow. The valve can be opened with a procedure called balloon valvuloplasty. This procedure is done during cardiac catheterization. A balloon at the tip of the catheter is inflated to widen the valve opening. Or the valve can be repaired or replaced with open heart surgery. The cardiologist will assess your child's condition and talk with you about treatment choices.
What are the long-term concerns?
All treatment choices for AS are done to relieve symptoms. This means that the aortic valve is not repaired. It will always be abnormal. You child may have more problems with the valve again in the future.
After treatment, most children with AS can be active. The level and extent of physical activity will vary with each child. They may not be able to do some contact sports, such as football. Check with the cardiologist about what activities are OK for your child.
Your child will need regular follow-up visits with a cardiologist for life. This is to make sure the valve doesn’t become blocked again or leak too much. Children with valve replacements are more likely to need more surgery in the future.
If your child has a bicuspid aortic valve
A bicuspid aortic valve has 2 leaflets instead of 3. The leaflet tissue may also be abnormally thick. This defect may or may not cause AS, so symptoms aren’t always obvious. It can often go undetected into adulthood. If the problem is diagnosed in childhood, treatment is only needed if the valve blockage gets worse over time, or if the part of the aorta above the valve (aortic root) becomes too enlarged. A child with a bicuspid aortic valve may be at higher risk of infective endocarditis. Even if the diagnosis is not made until adulthood, the valve may need replacement later in life.