A
B
C
D
E
F
G
H
I
J
K
L
M
N
O
P
Q
R
S
T
U
V
W
X
Y
Z
Back to Intro
Click a letter to see a list of medical procedures beginning with that letter.
Click 'Back to Intro' to return to the beginning of this section.
Respiratory Distress Syndrome (RDS) in the Premature Infant
RDS is a breathing problem common in premature babies. It shows up right after delivery or within the first few hours after birth. Your baby may be cared for in the NICU (neonatal intensive care unit) or in another part of the hospital.
What causes RDS?
RDS occurs because the lungs have not developed fully enough to produce a substance called surfactant. This substance is needed for normal breathing. When fresh air is breathed in, it travels through airways in the lungs to tiny air sacs (alveoli). Oxygen passes from the air sacs into the bloodstream. Waste air is then breathed out. Normally, surfactant helps keep the alveoli open after exhaling. That way, fresh air can be breathed in easily. But if the lungs contain little or no surfactant, the air sacs collapse after each breath. The baby has to work very hard to reopen them. Babies with RDS may not be strong enough to keep breathing without help.
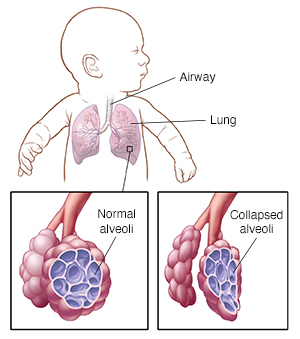 |
| Air travels through the airways (tubes in the lungs) to the alveoli (air sacs). Normally, alveoli stay open after each breath. RDS occurs when alveoli collapse after each breath. This means the baby has to work harder to breathe. |
How is RDS treated?
Treatments depend on how severe and persistent RDS is. They can include:
-
Artificial surfactant. This is often given through an endotracheal tube (ETT). This is a tube that goes through the baby’s mouth or nose into the windpipe. Or it may be given through a minimally invasive technique, such as a thin catheter in the windpipe or other route. More doses of surfactant may be given several hours apart.
-
Oxygen without ventilation. This is often given with a nasal cannula (soft tubes fixed under the baby’s nostrils). Or it can be given with an oxygen hood (clear plastic box that fits around the baby’s head). These devices give your baby oxygen without inserting tubes into the baby’s airway.
-
CPAP (continuous positive airway pressure). A CPAP machine provides continuous air flow into the baby’s airways. This helps keep alveoli from collapsing. CPAP may be used with or without supplemental oxygen.
-
Ventilator. This machine takes over some or all of the work of breathing. First, an ETT is inserted. The ventilator is then attached and used to send air into the lungs to help the baby breathe. To prevent damage to the lungs, the machine uses the lowest amount of pressure that works to fill the baby's lungs with air. The ventilator is used until the baby’s lungs are making surfactant and the baby is strong enough to breathe without help.
What are the long-term effects?
For many babies, RDS has no long-term effects. Even if alveoli are damaged, the baby is still able to grow new alveoli. If complications do occur, they can include:
-
Increased likelihood of developing asthma
-
Increased sensitivity to lung irritants
-
Increased risk for respiratory infections
-
Lung damage due to RDS or long-term ventilation. This can sometimes lead to bronchopulmonary dysplasia (persistent breathing difficulties). This may need long-term medicine, supplemental oxygen, or continued support with a breathing machine (ventilator).
Online Medical Reviewer:
Donna Freeborn PhD CNM FNP
Online Medical Reviewer:
Liora C Adler MD
Online Medical Reviewer:
Stacey Wojcik MBA BSN RN
Date Last Reviewed:
12/1/2022
© 2000-2024 The StayWell Company, LLC. All rights reserved. This information is not intended as a substitute for professional medical care. Always follow your healthcare professional's instructions.